Dog licking and losing hair: when the skin is the late expression of a systemic process
In brief Chronic licking and hair loss in dogs are rarely a primary skin disease. In most cases they are the late cutaneous expression of a systemic process —sustained stress, hypercortisolemia, and immunosuppression— that progresses subclinically for months or years before becoming visible.
If a dog has been licking, scratching, or losing hair for months —or years— and at every visit receives the same label («dermatitis») or the same presumed culprit («chicken allergy»), the problem is rarely where everyone is looking.
In daily clinical practice a consistent pattern recurs: patients with skin disease labelled for years as «dermatitis» or «food allergy», treated symptomatically with successive diets and shampoos, without any systemic evaluation. A very high proportion of them also share a recognizable behavioural phenotype —intolerance of separation from the owner, hyperattachment, sustained panting or vocalization throughout the consultation. That clinical coincidence, observed repeatedly, is the starting point of this analysis.
One principle organizes the approach: the skin does not generate the disease; it announces it. The correct diagnostic question is not «what does the skin have?» but «what process has the skin been expressing, and since when?».
Licking as a clinical sign, not an isolated behaviour
Clinical definition Persistent licking and scratching are neither a diagnosis nor a mere behavioural problem. Acral lick dermatitis is a multifactorial condition in which organic causes —allergic, parasitic, infectious, orthopaedic, or neurological— coexist with a compulsive component, and in which secondary infection perpetuates the itch–lick cycle.4
Attributing licking to «nerves» or «boredom» describes part of the phenomenon but rarely its origin. The dermatological literature establishes that acral lick dermatitis arises from multiple determinants and that its resolution requires identifying and treating both the primary cause and the secondary infections that sustain it.4 Its behavioural component has further been characterized as an animal model of obsessive-compulsive disorder, with documented response to selective serotonin reuptake inhibitors.3
Hence the first methodological error: choosing a single explanation. «It is allergy» and «it is nerves» are not rival hypotheses; they often coexist, and they are almost never the beginning of the clinical history. Licking is the visible end of a causal chain that must be reconstructed in reverse.
The pathophysiological cascade: sustained stress and hypercortisolemia
Mechanism Chronic stress persistently activates the hypothalamic-pituitary-adrenal (HPA) axis and keeps cortisol elevated. This prolonged exposure can be objectified by measuring hair cortisol, a validated biomarker of chronic stress in the dog.1,2

The link between behaviour and skin disease is biochemical: cortisol. Under chronic stress —separation anxiety, hyperattachment, sustained environmental overstimulation— the HPA axis remains activated and cortisol loses its physiological rise-and-fall rhythm, staying elevated for prolonged periods.
This exposure is quantifiable. Cortisol is incorporated into the hair as it grows, and hair cortisol concentration has been validated as a marker of prolonged stress —over weeks to months—: dogs with chronic skin disease have shown significantly higher concentrations than healthy animals.1 A long-term stress synchronization between dog and owner has also been described, such that the animal's cortisol load partly reflects the emotional environment of the household.2
A necessary methodological caveat: hair cortisol is, to date, a research and contextualization tool, not a test with a universal clinical cut-off for individual diagnosis. Its value lies in gauging cumulative exposure, not in establishing a diagnosis on its own. What matters is not an isolated figure, but the effect of that sustained hypercortisolemia on the organism over time.
Immunosuppression and opportunistic proliferation
Key finding Sustained hypercortisolemia depresses cell-mediated immunity and favours the proliferation of opportunistic organisms. Adult-onset demodicosis is a marker of underlying immunosuppression: in a series of 122 dogs, about 40% had a concurrent disease, with a statistically significant association with hyperadrenocorticism and hypothyroidism.5
Prolonged cortisol elevation attenuates the cell-mediated immune response —that is, the surveillance that keeps the animal's own microbiome in check. When that surveillance declines, previously contained organisms proliferate.
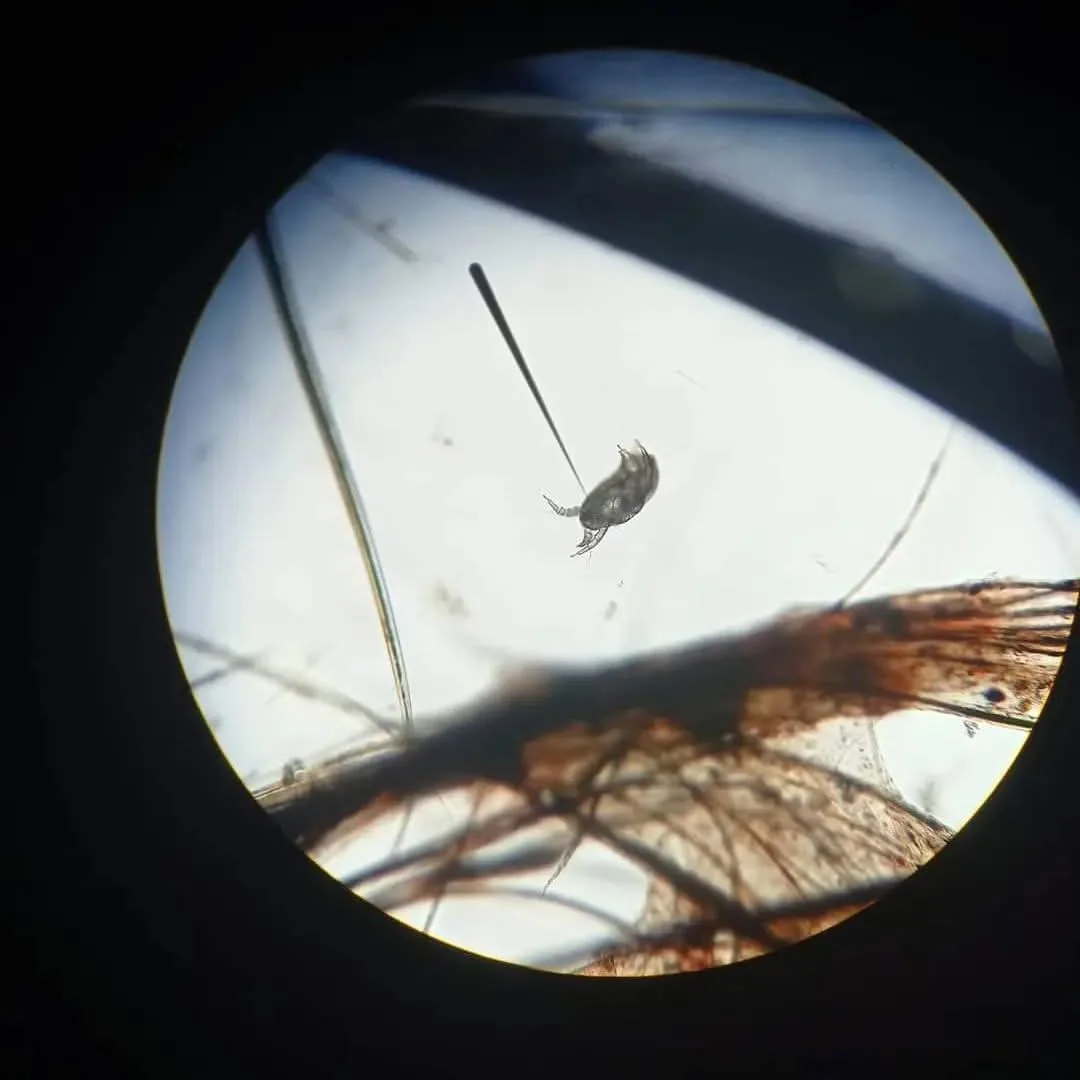
The paradigmatic example is Demodex. This mite is part of the dog's normal cutaneous fauna and coexists harmlessly while the immune system regulates it. The onset of adult-onset demodicosis —in a mature animal with no prior history— is therefore a warning sign of underlying immunosuppression. The reference study of 122 dogs with adult-onset demodicosis documented concurrent disease in about 40% of cases, with a significant association with glucocorticoid excess (hyperadrenocorticism) and hypothyroidism, and concluded that these patients should be evaluated systemically, not merely treated for the parasite.5
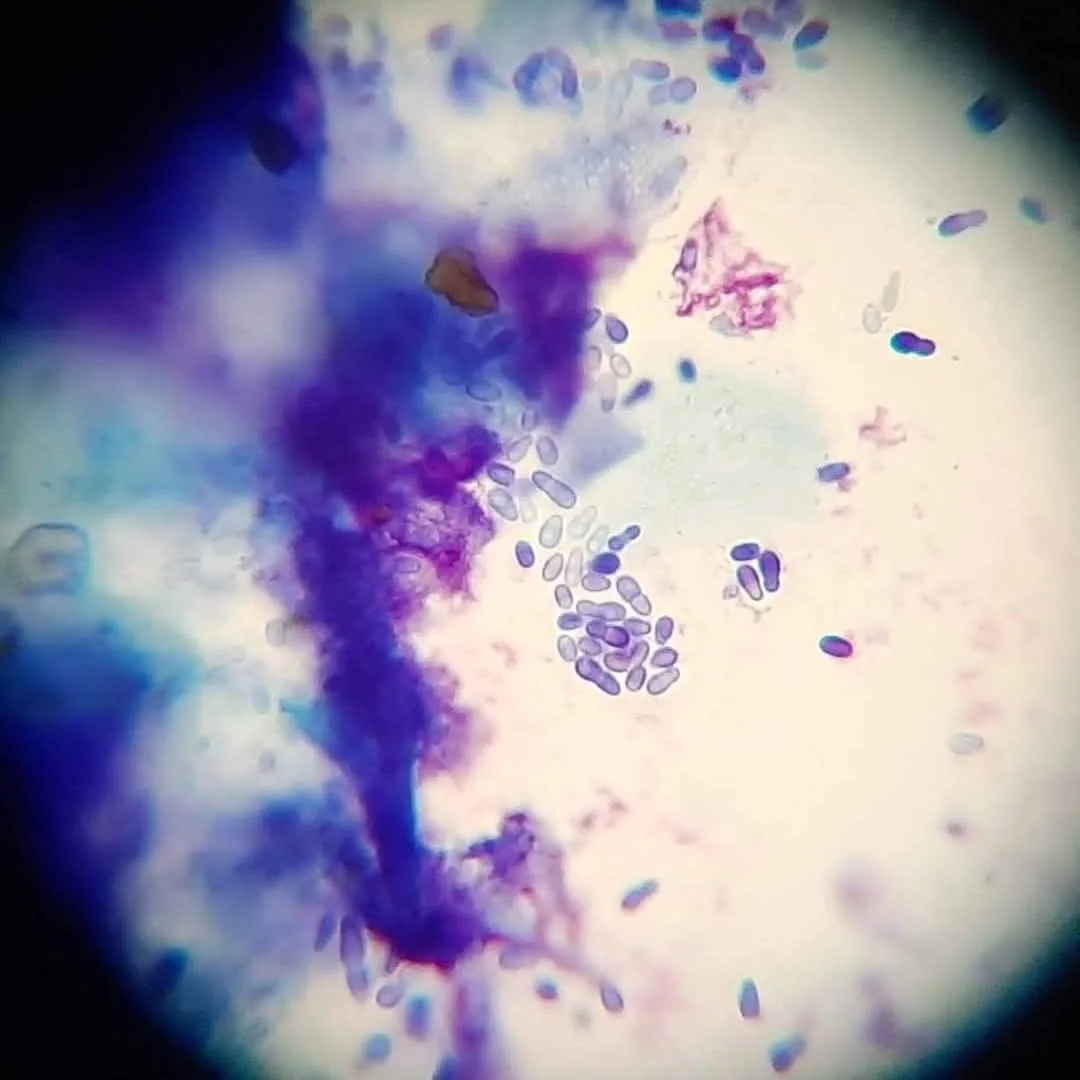
The same principle applies to Malassezia yeasts and bacterial pyoderma: they are opportunistic colonizers expressed on skin and immunity that are already compromised. International dermatology consensus guidelines state explicitly that effective treatment of Malassezia dermatitis requires identifying and correcting the predisposing disease.8 The yeast is not the origin of the condition, but the opportunist exploiting the immunosuppression.
The double endocrine deception: pseudo-Cushing and sick euthyroid
Diagnostic caution Hypercortisolemia of non-adrenal origin can mimic hyperadrenocorticism (Cushing's syndrome) and alter endocrine tests, producing false positives. For this reason, Cushing's and thyroid function tests should not be performed in a patient under stress or with uncontrolled concurrent illness.6,7
Pseudo-Cushing. Sustained cortisol elevation produces signs that resemble Cushing's syndrome —thin skin, alopecia, recurrent infections— but clinical resemblance is not diagnostic identity. True hyperadrenocorticism almost always has a defined organic cause (pituitary or adrenal neoplasia) and is confirmed by specific functional tests. Stress and non-adrenal illness can alter precisely those tests and produce false positives; for that reason, the ACVIM consensus advises against diagnosing Cushing's in a stressed dog or one with intercurrent disease.6 Chronic stress does not cause Cushing's: it mimics it, and demands a rigorous differential diagnosis.
Non-thyroidal illness syndrome. An analogous phenomenon affects thyroid function: a systemic illness or sustained stress can lower thyroxine (T4) concentrations without any primary thyroid disease. A recent study in acutely ill dogs documented total T4 below the reference interval in 100% of patients at admission, with spontaneous normalization within two to four weeks after recovery, without thyroid treatment.7 Interpreting thyroid function in the middle of a stress state, without context, leads to erroneous diagnoses of primary hypothyroidism and to unnecessary lifelong treatment.
Diagnostic method: the skin as a late interpreter
Protocol The correct approach reverses the sequence: the cutaneous sign is the last link in the chain, not the first. Behavioural and environmental history precedes the physical exam and the laboratory; and in the dog an organic cause must be ruled out before attributing the condition to a psychogenic origin.4
Diagnosing a patient that licks and loses hair is not about selecting a topical treatment, but about reconstructing the clinical history in reverse until the point of origin is identified. The assessment therefore begins with context, not with the lesion: timing and circumstance of licking, behaviour upon separation, sleep pattern, the real composition of the diet —not the one declared on the package— and social interaction. These variables are the first diagnostic instrument and turn the owner into an active informant of the process.
On that map the laboratory acquires meaning: skin scraping and cytology to identify the agent —mite, yeast, bacterium— and endocrine testing interpreted in context. One rule protects the patient: in the dog, before assigning a «psychological» origin, the organic cause must be ruled out. Strictly psychogenic alopecia is well characterized in the cat, but in the dog it is an entity with weak support; frequently, a physical cause amplified by stress underlies the licking. Stress is rarely the sole explanation, but it is almost always part of it.
When the behavioural component is real, it is part of the treatment plan together with environmental management and, in selected cases, pharmacological management under clinical judgment.3 Nonetheless, treating the anxiety while ignoring an underlying hyperadrenocorticism —or vice versa— again amounts to resolving only half of the condition.
Indication for systemic evaluation
When to seek evaluation Systemic evaluation is indicated when the skin condition is chronic or recurrent, responds only partially or transiently to dermatological treatment, and coexists with signs of stress, hyperattachment, or intolerance of separation.
When a skin condition persists over time, improves transiently with each treatment and recurs, and is accompanied by a behavioural profile of hyperattachment or sustained alertness, the dermatological lesion is usually the visible expression of a deeper process best evaluated as a system, not as a local sign.
The consultation format includes guidance and follow-up without geographical restriction: resolving the diagnostic question prior to an in-person consultation, advising on appropriate complementary tests, interpreting results already obtained, and supporting cases under treatment. When the case requires physical examination, referral to a trusted colleague in the patient's city is part of the service.
Veterinary consultation — Dr. Jessica Camacho García
Contact: [email protected] · Methodological framework: systemic veterinary diagnosis.
References
Peer-reviewed veterinary and biomedical literature. Each reference was independently verified at its original source (PubMed / publisher).
- Park SH, Kim SA, Shin NS, Hwang CY (2016). Elevated cortisol content in dog hair with atopic dermatitis. Jpn J Vet Res 64(2):123-129. PMID 27506086
- Sundman AS, et al. (2019). Long-term stress levels are synchronized in dogs and their owners. Sci Rep 9:7391. doi:10.1038/s41598-019-43851-x
- Rapoport JL, Ryland DH, Kriete M (1992). Drug treatment of canine acral lick. An animal model of obsessive-compulsive disorder. Arch Gen Psychiatry 49(7):517-521. doi:10.1001/archpsyc.1992.01820070011002
- Shumaker AK (2019). Diagnosis and Treatment of Canine Acral Lick Dermatitis. Vet Clin North Am Small Anim Pract 49(1):105-123. doi:10.1016/j.cvsm.2018.08.010
- Pinsenschaum L, Chan DHL, Vogelnest L, Weber K, Mueller RS (2019). Is there a correlation between canine adult-onset demodicosis and other diseases? Vet Rec 185(23):729. doi:10.1136/vr.105388
- Behrend EN, et al. (2013). Diagnosis of Spontaneous Canine Hyperadrenocorticism: 2012 ACVIM Consensus Statement. J Vet Intern Med 27(6):1292-1304. doi:10.1111/jvim.12192
- Bolton TA, Panciera DL, Voudren CD, Crawford-Jennings MI (2024). Thyroid function tests during nonthyroidal illness syndrome and recovery in acutely ill dogs. J Vet Intern Med 38(1):111-122. doi:10.1111/jvim.16947
- Bond R, et al. (2020). Biology, diagnosis and treatment of Malassezia dermatitis in dogs and cats: Clinical Consensus Guidelines of the WAVD. Vet Dermatol 31(1):28-74. doi:10.1111/vde.12809

Dr. Jessica Ysabel Camacho García
ORCID 0009-0002-6837-5311 · Professional verification · Last reviewed: 19 June 2026